ALWAYS control for population variance if you want to better understand the influence of the health system on outcomes:
Here is what I wrote in another thread about breast cancer:
Breast cancers are not all the same in how they develop. One key difference is found in
Estrogen Receptors:
Receptors for the female hormones estrogen and progesterone are another key personality feature of breast cancer.
These receptors are the eyes and ears of the breast cells, getting messages sent by the hormones and figuring out what to do with these messages. The hormones will tell the receptors to stimulate or "turn on" breast cell growth. Estrogen and progesterone can increase both normal and abnormal breast cell growth.
If a tumor is estrogen-receptor positive (ER-positive), it is more likely to grow in a high-estrogen environment. ER-negative tumors are usually not affected by the levels of estrogen and progesterone in your body. This is one time when hearing the word "positive" may really mean something good.
As ER-positive cancers are more likely to respond to anti-estrogen therapies. If you have an ER-positive cancer, you may respond well to tamoxifen (Nolvadex), a drug that works by blocking the estrogen receptors on the breast tissue cells and slowing their estrogen-fuelled growth
The question that needs to be asked is whether there is population variance seen for the distribution of ER+ and ER- breast cancers.
Oh oh, there is population variance. Now the question shifts to
"what does this mean?"
Black women may be at increased risk for aggressive, difficult-to-treat triple-negative breast cancer, independent of their age and weight, researchers found.
Tumors that did not express estrogen or progesterone receptors or HER2 were three times more common among black women than among white women (P=0.0001), Carol L. Rosenberg, M.D., of Boston University Medical Center, and colleagues reported online in Breast Cancer Research.
The effect of race or ethnicity in the single center cohort did not vary with age and body mass index, suggesting that triple-negative disease "likely contributes to black women's unfavorable breast cancer prognosis," the researchers said.
Black women in the U.S. have an overall lower risk of developing breast cancer overall than their white peers, but their cancers are diagnosed at a higher stage, with a greater risk of recurrence and worse prognosis.
Prior studies have found a higher rate of triple-negative breast cancer in minorities including blacks. . . .
Overall, 20% of the women had triple-negative tumors while 72% expressed estrogen, progesterone, or both types of receptors. Some 13% were HER2 positive.
However, triple-negative breast cancer was not evenly distributed among racial and ethnic groups. Black women had a 30% rate of these aggressive tumors compared with just 11% to 13% in the other groups.
In a multivariate regression analysis, triple-negative status was three times more likely among black than white women (95% confidence interval 1.6 to 5.4).
So, when black women develop breast cancer they tend to develop a more aggressive type which is more difficult to treat and which results in higher rates of mortality. International comparisons on breast cancer treatment outcome don't account for this at all. What's happening with a US-Norway comparison on breast cancer treatment outcomes is not a comparison of the financing systems of the two countries, but a comparison of white Norwegian women being treated successfully for predominantly ER+ breast cancers and US women, who are a mix of white women suffering from ER+ breast cancer with a more successful treatment regime in place and black women who have higher rates of ER- breast cancers which are more aggressive and result in higher mortality, and the outcomes for both groups (I'm leaving out Asian, Hispanics, Natives, etc just to simplify the point here) are mashed together and we look at American outcomes and then we presume that the difference in mortality arises from how we structure our health care model.
Breast cancer is just one example of how population variance skews international health comparison reports. Disease related population variance is seen for most diseases. This is why you need to control for population variance in these international comparisons, and that's not just for health reporting, you need to do it for things like poverty, for infant mortality, for educational outcomes, for crime, etc. Compare Norwegians to Norwegian Americans and you get a better understanding of how social programs, the focus of your study, are affecting outcomes. Don't do that and all you get is gibberish.
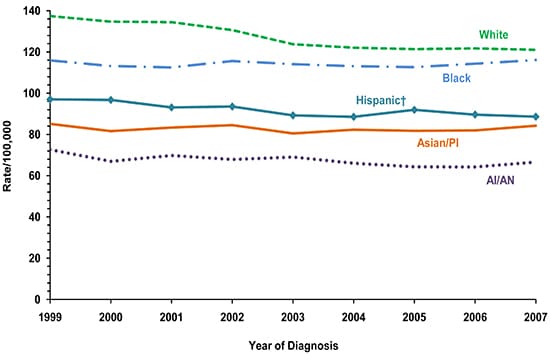
Two graphs from the
CDC on Breast Cancer incidence rates and mortality