No, lower. Thanks to the wonderful laboratory of Democracy, we actually have an increasingly good idea of what kinds of reforms
are capable of reducing costs (or, at least, holding them steady) while continuing to provide equal or greater actual
health care.
The chief problem with our current healthcare system is an abundance of awkward and disruptive government interference. This has led to the dominance of a third-party-payment model which discourages cost-awareness and encourages over-consumption among health care consumers. Government pays for roughly half of our healthcare consumption, and of all third-party payment options, government is the one
least likely to be capable or willing to nimbly find ways to impose cost awareness on those capable of sending it bills. The result is a healthcare system in which costs rapidly spiral out of control (we have a similar problem in our higher education industry). Any system which does not alter that disruption and incentivize cost-awareness among consumers for the vast majority of medical purchases will not address the chief underlying flaw of our current system, and we will continue to see costs spiral outside of the control of the citizenry and government.
Reforms which
have pushed cost-awareness back onto consumers have demonstrated impressive results at lowering expenditures:
Indiana offered HSA's, - which have patients save money in tax-free accounts (where it grows and remains theirs forever and ever unless theys pend it) - matched with high deductible plans to it's employees. Employees began to respond to price signals, and medical costs per patient were reduced by 33% and expenditures to the state were reduced by 11%.
Safeway has instituted a program that gave financial incentives to people who engaged in healthy behavior by allowing price signals in the
insurance side of the market to work (Indiana worked on the medical side), and saw it's per-captia health care costs remain flat from 2005-2009; when most companies saw theirs jump by 38%.
Whole Foods instituted HSA's, and let's the employees choose what they want the company to fund. This institutes price pressure on the medical side (WF covers the high-deductible plan 100%), and their CEO points out that as a result Whole Foods' per-capita costs are much lower than typical insurance programs, while maintaining employee satisfaction.
Medicare Part D utilized market pressure on the insurance side, and saw expenditures come in at 40%
UNDER expenditures - the only such government program in history to do so.
Wendy's instituted HSA's, and saw the number of their employees who got preventative and annual checkup care climb even as they saw claims decrease by 14% (in one year).
Wal-Mart's low cost clinics and prescriptions save us oodles of cash. Wal-Mart reports that "half of their clinic patients report that they are uninsured" and that "if it were not for [Wal-Marts'] clinics they would haven't gotten care - or they would have gone to an emergency room".
Dr Robert Berry runs a practice called PATMOS (payment at time of service). he doesn't take insurance at all - but simply posts the prices of his services. By removing the cost of dealing with mutliple insurance agencies, medicare, and medicaid, the prices he is able to list are one half to
ONE THIRD of industry standard.
So we know what works, because we've seen it. It's simply that implementing what works means less power in our nations capitals, which means less cash for our nations' politicians, which means less support for implementing it in the first place.
Oh, we'll just magically "reroute" it. :roll: sure. We'll hit the "reroute" button because people treat purchasing goods and services
exactly the same way they treat paying taxes.
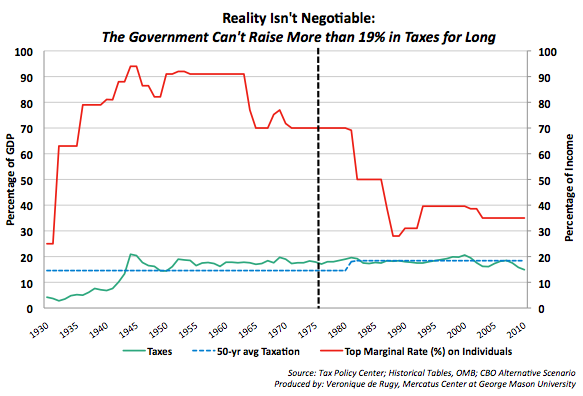
Yeah, raising taxes. Except as I've already demonstrated, never in the history of our country have we raised enough taxes to "reroute our spending" into the federal coffers. You're simply not going to get it, especially once you factor in the fact that when you raise the cost of employment by (for example) 9%, you reduce demand for employees. These people think that making rates higher by 9%-15% would fund UHC? When our rates were
60 % higher we didn't raise enough to fund UHC.
But I'm open to being convinced. Average revenues in the pre-Great Recession Era were about 18.5% of GDP. If you can describe for me a single tax structure in American history that collected 6% of GDP over that amount for a 5 year period, I will re-assess my statement on the utter implausibility of the pie-in-the-sky notion that we can afford a massive new entitlement program.

")